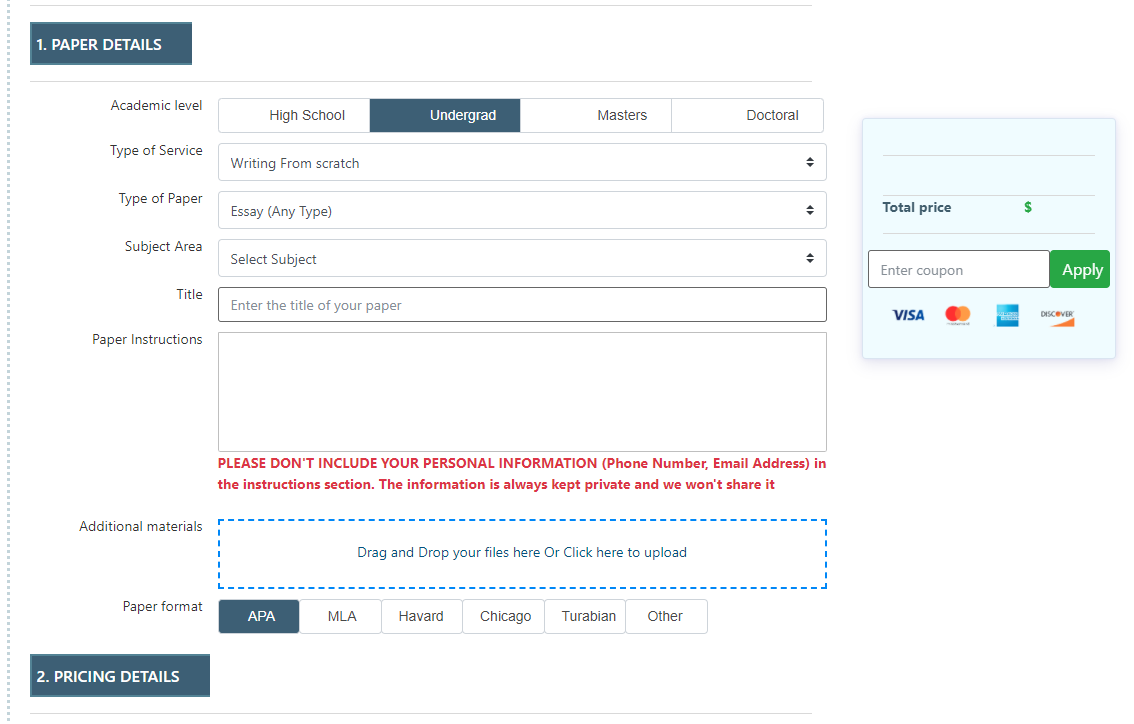
Fill out order details and instructions, then upload any files or additional materials if needed. Then, confirm your order by clicking “Place an Order.”

Read the feedback and look over the ratings to choose the writer that suits you best.

Check the inbox for notifications, download the completed assignment, and then release the payment.